On Monday of this week, I blogged about the Affordable Care Act (ACA) and what it might mean for non-profit organizations including those that have fewer than 50 employees and don’t think this legislation applies to them. At the end of my post, I asked a few questions as I always do. Within 24 hours, one person did weigh-in and others sent me direct emails. So, I decided to share that expert feedback with you today.
Feedback from a federally qualified healthcare center
 The following is a comment from Rose Reinert who is a community outreach liaison from a healthcare non-profit in my hometown of Elgin, Illinois. I’m sharing it here because I know many of you don’t get an opportunity to loop back around to former posts to read the comments.
The following is a comment from Rose Reinert who is a community outreach liaison from a healthcare non-profit in my hometown of Elgin, Illinois. I’m sharing it here because I know many of you don’t get an opportunity to loop back around to former posts to read the comments.
Great post Erik! As you know, I work as Community Outreach Liaison for an area Federally Qualified Health Center that meets the medical and dental needs of all, regardless of ability to pay, and I can say there are a lot of changes coming. It reminds me of when we used to play hide and seek and scream, “Ready or not! Here I come!” In this case, we have to make ourselves ready, and there are a lot resources to do so.
I have also found a lot of confusion surrounding the Affordable Care Act. Having said that, our organization, Greater Elgin Family Care Center has received federal and state funding for In Person Counselors who can assist in education and enrollment.
If anyone is in the Greater Elgin area and would like to learn more about the Affordable Care Act, please let me know. We can come to you to give talks to your staff, your clients, or any one who might want to learn more!
Rose Reinert, rreinert@gefcc.org
Feedback from an HR professional
 The following is an email from a former volunteer and friend of mine who is a human resources professional. Her comments reference resources she recently blogged about. (I should note that she is one of my favorite HR bloggers and I subscribe to her site) If you want to check out her blog, click here to visit her site which is titled “Don’t bite the apple . . . Work is not a fairytale”.
The following is an email from a former volunteer and friend of mine who is a human resources professional. Her comments reference resources she recently blogged about. (I should note that she is one of my favorite HR bloggers and I subscribe to her site) If you want to check out her blog, click here to visit her site which is titled “Don’t bite the apple . . . Work is not a fairytale”.
Here is what she said in her email:
Erik,
Hi there, I hope all is well. Great Article on Obamacare. I didn’t want to post my blog to yours and some of my information doesn’t apply. I just wrote a post on the notices with a link to the DOL approved notices.
ALL businesses subject to FLSA (which is pretty much everyone) has to send notices to employees to tell them if they are or are not providing insurance by October 1st. It has to go to ALL employees f/t, p/t and even if not on insurance. It’s a great thing to post about and provide the links. The first page of the notices explain to the employees how to go out to exchanges and look at healthcare. It also notifies people that if they buy from there and the employer pays part of the premium they can lose their match.
Feel free to take anything you’d like out of the post and if you need anything else, I’d be happy to help. I have access to a lot of info through SHRM.
Have a great day,
Denise
Feedback from an insurance professional
 Dan Walter is a board member for my local United Way and he is a partner and senior vice president for Lundstrom Insurance. After reading Monday’s blog post, he sent me a guest commentary he recently wrote for The Daily Herald newspaper.
Dan Walter is a board member for my local United Way and he is a partner and senior vice president for Lundstrom Insurance. After reading Monday’s blog post, he sent me a guest commentary he recently wrote for The Daily Herald newspaper.
Here is his article about the Affordable Care Act:
The Affordable Care Act (ACA) is about to enter its most far-reaching phase. In 2014, the ACA mandates that nearly all citizens purchase qualifying health insurance or pay a penalty. Guaranteed insurability will provide access to health insurance coverage regardless of health history. Health plans must accept pre-existing conditions that might have been denied or limited under the present rules.
The Health Insurance Marketplaces, also known as the public Exchanges, are scheduled to be operational on October 1st, with coverage that can be effective as soon as January 1, 2014. Rather than create its own exchange, Illinois chose to partner with the exchange established by the federal government. Illinois consumers will have access to six carriers, far fewer than originally anticipated.
By October 1st of this year, most employers are required to distribute a notice to every employee informing them about the Health Insurance Marketplace. The Marketplace/Exchange will provide access to private health insurance plans as well as certain government-based health plans like Medicare and Medicaid. Also, the public Marketplace/Exchange is the only place an individual can access premium and cost-sharing subsidies. Premium subsidies are available on a sliding scale up to 400% of the federal poverty level (FPL) and consider the entire household income for eligibility. Cost-sharing subsidies help offset high out of pocket costs for people with incomes up to 250% of the FPL.
Insurance will continue to be available through brokers and carriers without going through the Marketplace. Brokers will have access to many other plans and other carriers, as well as those on the Marketplace/Exchange. Some carriers like Blue Cross Blue Shield of Illinois have also created their own private health insurance exchanges which brokers can access on behalf of their clients.
New ACA Fees and taxes will also go into effect in January. Two of these new costs are the Health Insurer Fee and the Reinsurance Fee. Starting at $8 Billion in 2014, the Health Insurer Fee will apply to health insurers offering individual coverage and fully insured group plans. The tax is allocated among health insurers based on relative market share. By 2018 this tax will have grown to $14.3 Billion.
The Reinsurance Fee is scheduled to be in effect for a three year period, decreasing over that time from a starting point of $5.25 per person, per month and applies to individual coverage and fully insured group plans, as well as self funded plans.
Combined, these two fees will add an estimated 3-4% to the premium. The amount will vary based on the number of people covered and a formula applied to the carrier’s net premium for the prior year.
In July of this year it was announced that the penalties and reporting requirements of the so-called “Employer Mandate” would be delayed to 2015. This portion of the law affects businesses with 50 or more full time equivalent employees and obligates them to offer coverage that meets certain standards of coverage and premium affordability. Not doing so will risk fines ranging from $2,000 per full time employee, to $3,000 for each full time employee who obtains a subsidy on the government Marketplace/Exchange. Other requirements and timelines of the ACA remained intact.
This is only a brief summary of some key points of ACA. If this sounds confusing or complex, it reinforces why individuals and businesses should be very discerning about ACA related information. Be sure to identify whether the information you rely on applies to individuals, small or large employers, and even whether it applies to your state or not. Obtain good counsel and guidance to help you understand your choices as well as your compliance obligations and potential penalties.
The impact of ACA is far reaching. With appropriate guidance, you will navigate it just fine.
My final thoughts on this issue
If you think your non-profit won’t be impacted by ACA, you are most likely wrong. At a minimum, this legislation will get your employees talking about healthcare benefits in your workplace. It would be wise to read up on ACA, talk to your insurance people, and be prepared to talk intelligently with your employees about this issue if and when questions arise.
This blog thread appears to have resonated with DonorDreams readers. Do you have more questions or comments? If so, please use the comment box below to share your thoughts and experiences.
Erik Anderson
Founder & President, The Healthy Non-Profit LLC
www.thehealthynonprofit.com
erik@thehealthynonprofit.com
http://twitter.com/#!/eanderson847
http://www.facebook.com/eanderson847
http://www.linkedin.com/in/erikanderson847
 Full discloser . . . I went out for a few glasses of wine on Tuesday night with a non-profit friend and got back home a little late at night. So what? Who cares? Well, I need to be up and on the road at 5:00 am to visit an out-of-state client, which means I needed to write my Wednesday blog post on Tuesday night. Oooops! So, I’m heading to bed in the next few minutes and wringing my hands about not writing something in the morning. Luckily, my friend said something provocative over a glass of wine and that will the be center of today’s post.
Full discloser . . . I went out for a few glasses of wine on Tuesday night with a non-profit friend and got back home a little late at night. So what? Who cares? Well, I need to be up and on the road at 5:00 am to visit an out-of-state client, which means I needed to write my Wednesday blog post on Tuesday night. Oooops! So, I’m heading to bed in the next few minutes and wringing my hands about not writing something in the morning. Luckily, my friend said something provocative over a glass of wine and that will the be center of today’s post. I am not a healthcare expert, and I promise not to play one today. However, the Affordable Care Act (aka Obamacare) has been mentioned in passing a handful of times in meetings I’ve had with non-profit board and staff members over the last few months. Of course, when things like this happen, it tweaks my curiosity and normally ends up here as a blog post. Today, I thought I’d quickly touch upon the quickly evolving topic of healthcare and the non-profit sector and how everyone needs to start paying attention.
I am not a healthcare expert, and I promise not to play one today. However, the Affordable Care Act (aka Obamacare) has been mentioned in passing a handful of times in meetings I’ve had with non-profit board and staff members over the last few months. Of course, when things like this happen, it tweaks my curiosity and normally ends up here as a blog post. Today, I thought I’d quickly touch upon the quickly evolving topic of healthcare and the non-profit sector and how everyone needs to start paying attention. Why?
Why? Welcome to O.D. Fridays at DonorDreams blog. Every Friday for the foreseeable future we will be looking at posts from John Greco’s blog called “
Welcome to O.D. Fridays at DonorDreams blog. Every Friday for the foreseeable future we will be looking at posts from John Greco’s blog called “ The point I’m trying to make is that most non-profit organizations have built a culture that revolves around THE CLIENT. This focal point is so intense that ideas threatening to shift that focus are often seen as heresy.
The point I’m trying to make is that most non-profit organizations have built a culture that revolves around THE CLIENT. This focal point is so intense that ideas threatening to shift that focus are often seen as heresy.
 The following is a thumbnail sketch of what my process looked like:
The following is a thumbnail sketch of what my process looked like: I am not suggesting that my process is the right way to put a non-profit budget together. However, I do believe strongly in the following few budget construction principles:
I am not suggesting that my process is the right way to put a non-profit budget together. However, I do believe strongly in the following few budget construction principles: You know what Douglas Adams says (according to
You know what Douglas Adams says (according to  When I look at my email inbox, I do a lot of scanning. I first look at the names of people who sent me something. As I do this, I am deleting anything that vaguely looks like spam or advertising. I don’t even open it. After this first purge, I re-visit those who are left standing and start looking at subject lines. I’m essentially trying to prioritize what I should open first versus leave for later when I have more time. And when I say “leave for later,” it could be days or weeks later.
When I look at my email inbox, I do a lot of scanning. I first look at the names of people who sent me something. As I do this, I am deleting anything that vaguely looks like spam or advertising. I don’t even open it. After this first purge, I re-visit those who are left standing and start looking at subject lines. I’m essentially trying to prioritize what I should open first versus leave for later when I have more time. And when I say “leave for later,” it could be days or weeks later. Every year, it seems like one of the charities I support is celebrating some kind of anniversary or milestone. Most of the time, it relates to the age of the organization, and it is typically a milestone like 25, 50, 75 or 100 years of existence. Sometimes it is a different kind of anniversary, where they’re celebrating a board member’s years of service or the age of something physical like a building. Regardless of the opportunity to celebrate, a fundraising solicitation is never far behind; however, anniversary celebrations can be so much more than just putting your hand out.
Every year, it seems like one of the charities I support is celebrating some kind of anniversary or milestone. Most of the time, it relates to the age of the organization, and it is typically a milestone like 25, 50, 75 or 100 years of existence. Sometimes it is a different kind of anniversary, where they’re celebrating a board member’s years of service or the age of something physical like a building. Regardless of the opportunity to celebrate, a fundraising solicitation is never far behind; however, anniversary celebrations can be so much more than just putting your hand out. A few weeks ago, I started getting email and snail-mail announcing the 100th anniversary of the
A few weeks ago, I started getting email and snail-mail announcing the 100th anniversary of the  For example . . .
For example . . . As with most things in this world, there are different schools of thought on different things. While working with a client recently, I was reminded of the two camps that non-profit professionals tend to fall into when it comes to writing vision statements. So, I thought it would be fun this morning to explore both perspectives.
As with most things in this world, there are different schools of thought on different things. While working with a client recently, I was reminded of the two camps that non-profit professionals tend to fall into when it comes to writing vision statements. So, I thought it would be fun this morning to explore both perspectives. Welcome to O.D. Fridays at DonorDreams blog. Every Friday for the foreseeable future we will be looking at posts from John Greco’s blog called “
Welcome to O.D. Fridays at DonorDreams blog. Every Friday for the foreseeable future we will be looking at posts from John Greco’s blog called “ One of the pre-test questions that tends to trip people up is whether or not the board has a responsibility to “oversee the CEO“. Believe it or not, it isn’t uncommon for one-quarter to one-third of board volunteers to say “NO“.
One of the pre-test questions that tends to trip people up is whether or not the board has a responsibility to “oversee the CEO“. Believe it or not, it isn’t uncommon for one-quarter to one-third of board volunteers to say “NO“. So, maybe you don’t know where to start?
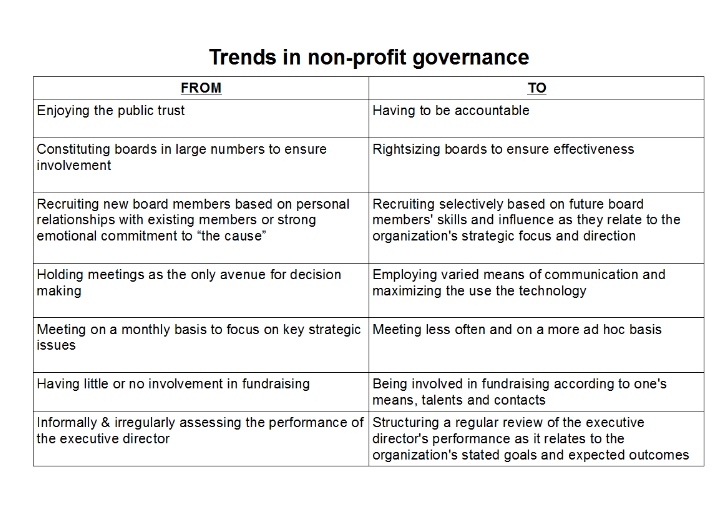
So, maybe you don’t know where to start? I was reviewing some old non-profit board governance material this morning and came across a document talking about “trends in non-profit governance“. In other words, the person who wrote that paper thought s/he was able to predict the future. Of course, this document was written more than 10 years ago, which got me thinking it might be fun to review some of their trends and determine where they were right or wrong.
I was reviewing some old non-profit board governance material this morning and came across a document talking about “trends in non-profit governance“. In other words, the person who wrote that paper thought s/he was able to predict the future. Of course, this document was written more than 10 years ago, which got me thinking it might be fun to review some of their trends and determine where they were right or wrong.